Statistics
Beyond Blue uses statistics from trusted references and research.
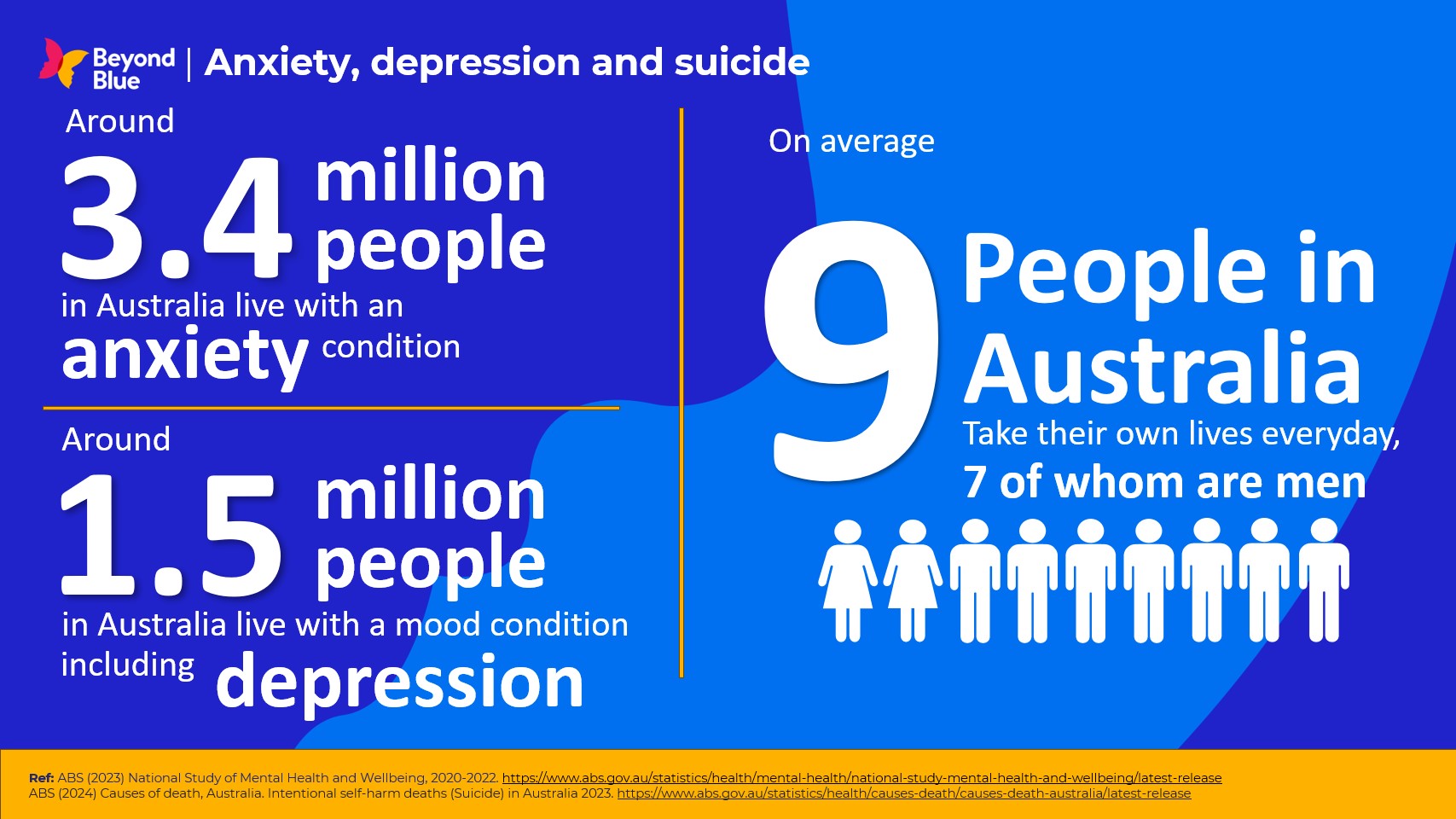
View some of our most commonly used stats, or find the relevant category from the list below to find the specific information you're looking for.
Beyond Blue uses statistics from trusted references and research.
View some of our most commonly used stats, or find the relevant category from the list below to find the specific information you're looking for.
As an organisation that supports people from across Australia, Beyond Blue acknowledges the Traditional Owners and Custodians of Country and their continuing connection to land, waters and community. We pay respect to Elders past and present.
First Nations Peoples are advised that this website may include reference to and images of deceased persons.
Beyond Blue is committed to safe inclusive spaces, policies and services for people of LGBTIQ+ communities and their families.
Premier partners

